Topics Discussed Include the Following...
*Treating alopecia in women undergoing chemotherapy for breast cancer
*Treatment algorithm for erectile dysfunction
*Vacuum Pump for Penis--science
*What etiologies for ED are best treated with the P-Shot® procedure?
*Tips for interviews on the news, podcasts, and magazines
Video/Recording of CMA Journal Club, Pearl Exchange, & Marketing Tips
Relevant Transcript, Relevant Research, Relevant Links
Transcript
Welcome to the Journal Club. We have four main topics for the night, hope you guys will jump in. In the end, I'll cover a question. For two days in a row, it usually happens about once or twice in a month, but now two days in a row have had text messages with questions from people who are being interviewed about our P-Shot® procedure on the news or a podcast somewhere, and still seems like our popularity of the procedure's growing. So I thought I would cover some of those commonly asked questions and some tips about how to deal with the news if you're on the news or in someone's podcast or webinar. How to direct the questions so that you are in control and yet honestly deal with both concerns and benefits of what we do. That will come last. Also wanted to cover some research regarding vacuum devices. There was a nice review article that came out about treating erectile dysfunction in those who suffer from diabetes, and the pump came up in that article. So I thought I'd review that.
And then there was a nice paper looking at the treatment of alopecia and those who are undergoing chemotherapy specifically for breast cancer. And I thought that would be interesting. So those are the topics for the night. Why don't we start with the chemotherapy article?
Treating alopecia in women undergoing chemotherapy for breast cancer
Okay, hold on a second. There we go. Specifically, the question I get repeatedly is what about PRP and those who are undergoing chemotherapy?
This article has to do more with while people are in the process of receiving their chemotherapy, this is a huge problem. Research shows us one of the major disturbing things about undergoing chemotherapy, especially for women, is the loss of their hair. And so, is there something we can do to help prevent it?
The main thing I wanted to show you here is yes, there are scalp-cooling devices that have been approved by the FDA for this purpose. Actually, let me go ahead before I go further and give you a link to this article, and I'll put this in the chat box.
But the main gist of what I wanted to show you is that when they looked at preventing it during therapy, PRP was not so hot. And that has been my observation as a matter of fact, you can read it right there. Whereas host dermal collagen, endogenous thrombin are able to activate PRP calcium gluconate. Oh that's just talking about the activation. And many of the studies leave that off. So I wanted to make sure you see that in my opinion, if they're studying are especially or sexual dysfunction procedures, they should be activating. This is what I was getting at in the rat model, it didn't help. And my recommendation is you wait until people are through with their therapy. Because the general rule of thumb that I go by and when I use platelet-rich plasma is if your body is in a catabolic state, then it's going to attenuate possibly completely block the benefits of platelet-rich plasma. All on the other hand have had great results in helping people regrow their hair after they finish the chemotherapy.
Whether it's making it come back faster or not. I think it is, they think it is. I tell them that without the PRP, it would eventually come back, but we can help it along if they want. All the rest of it, you can read it. But the bottom line is, in my opinion, you're left with pretty much the cooling devices, and then afterward, then you do everything you know to do. Otherwise, I think you'll be frustrated.
A treatment algorithm for those with ED and diabetes
Okay, that's the first thing I wanted to cover. Let me see if anyone has questions or comments about that. Because I am not an oncologist, I've just seen and heard from our providers that they are usually not helpful. Don't see any comments. So let's jump to the next topic, which is this review article that came out. Let's see this one. This one. I love this article because although I think it isn't absolutely complete, it's still helpful, especially for the primary care people in the group or if you're doing primary care as part of your gynecology or urology practice for women and men.
To back up a step, I honestly think that I could take a reasonably attentive 14-year-old and teach them to Botox the glabella and they would get pretty much 100% results, and they wouldn't have to know much of anything else. I don't think that's the case with treating sexual dysfunction. I don't think you have to be Tinsley Harrison or William Osler, but I do think to do it successfully requires an understanding of general medicine. And even if you're not going to do some of what's required, at least understand that certain things need to be done.
If you're going to do the procedure, at least have some idea of everything else that should be done, not just doing P-Shot®s. Otherwise, unlike treating the glabella, I think you'll have frustrated patients.
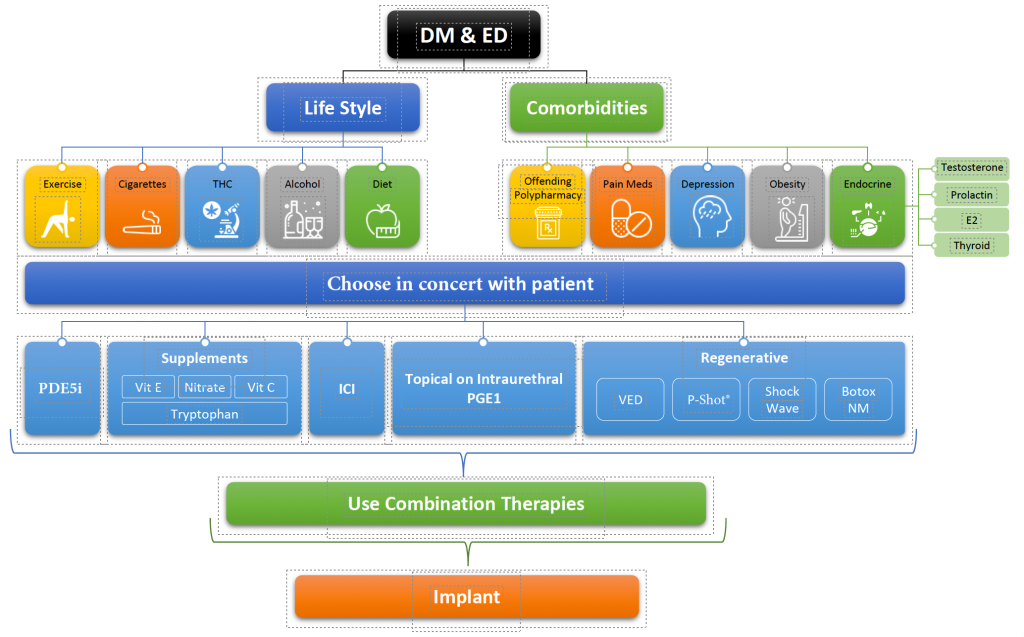
So this is really nice, this is an open-source article, so I'll give you the link to it, and you can download it. Hold on a second. Let me do that before I go further. Remember, if you click these buttons before I shut down the webinar, they'll be there. If you wait until the webinar's over, the link goes away. So basically, the idea was, how to manage ED and people with diabetes that are not responding to PD5Is. I would, and if you go down, they talk about comorbidities, complications from the comorbidities, you've got the metabolic syndrome, obesity, dyslipidemia, hypertension, hypogonadism, depression, polypharmacy or go along with those, that metabolic syndrome. And then there's a nifty little chart algorithm for the treatment.
And I would like to propose some mild modifications of this in that, maybe not everybody wants to go straight to PD five inhibitor. For example, it's hard to do, but when someone has type two diabetes or hypertension, unless something's changed, I don't know about, I think in the early stages, lifestyle modification is supposed to be the first thing to do.
And so this basically assumes that you start off with the PD five inhibitors and then if that's not helpful, you do the lifestyle thing. So I've included everything on this chart, but just made some modifications, and I'll show you the rest of it, and then I'll show you the modifications. And you guys correct me to add to whatever as we go along.
So it's to ensure they're using the medicine properly and then optimize the comorbidities. And then take a tailored approach, patient-centered care. In other words, you're going to do what good doctors do and listen to your patient. Maybe some of them aren't interested in taking supplements and the pump makes them feel like they're on a comedy show and they want to go straight to regenerative therapies and try your P-Shot®. Or maybe they have a friend and that's getting great results with injectable trimix and you go there.
Maybe you, there's a lot of expertise within physicians too. Maybe you have lots of experience with the intra urethral prostaglandin and that's your first choice. But the idea is you pick the best thing here and then combine them based on the results you get. And of course that would be the third step. Some synergistic combination of therapies. And fourth step would be penile prosthesis insertion.
So of course in this novel therapies, they put stem cells in shock wave, but they left out Botox and PRP, which as stem cells are not even available in the US. But if you look at a lot of these studies come out of like, this is Greece and London and maybe they don't have to worry about the FDA as much.
But here's the modification I made and not much was modified. I respect what they did. But trying to take more of a lifestyle change approach, at least incorporating it from the very start along with, and instead of just slamming with them with the Viagra to start with, there's a growing body of research about, they're not benign, these PDE5 inhibitors, you have blindness, you have strokes, and although there's some evidence that might help with prevent dementia and help with your knee retention and from prostate enlargement, but whatever, I just redesigned this and said diabetes associated with ED and of course this could be ED because the same changes happen in those who are just suffering general erectile dysfunction associated with aging. So the lifestyle, I expanded his list of lifestyle changes.
Exercise alone has been shown to increase erections seven points on the erectile dysfunction score, of course, cigarettes. And one thing that's not talked about but recreational marijuana can change some of the endocrine function. And I've seen that associated with higher estrogen levels, low testosterone, of course, alcohol and diet.
I think although alcohol is great to cause a loss of inhibition, I think it's responsible for also loss of erection. Just people get sleepier and not as erect. Anyway, the comorbidities also expanded that you have, of course, obesity, depression, I added in pain meds because I've seen that a lot. Maybe I'm somewhat biased because I've worked at pain clinics in the past and helped detox quite a number of people. But almost always, if they're on chronic pain medicines, they're LH and FSH drop and they're essentially castrated at the pituitary level and are going to almost always need some testosterone or something thrown in. I hesitate to treat chronic pain patients often cause their hormones are goofed up and oftentimes they're not as compliant. But that may be biased, but for sure, think about LH and FSH and testosterone levels. Of course offending polypharmacy, beta blockers classically.
And when it comes to depression medicines, I think most of you guys know I like swapping over to Wellbutrin and off of the SSRIs, oftentimes you come off of the antidepressant completely if they implement the exercise. On the endocrine level, the chart just listed testosterone. If you check for it, you'll find one or two per year who have hyperprolactinemia from a micro adenoma and you block them back with Destinex and they love you. And oftentimes that's all you have to do.
I had a UPS man that called on our office that was young and strong and impotent and I did... He asked me to take care of him and as he was dropping off his boxes one day drew his lab work and he came back in and all he needed was, he had a micro adenoma, nothing on MRI, just hyperprolactinemia. And you'll oftentimes see in the book, no reason to check that unless they have other pituitary hormone abnormalities.
But I just have found that to be wrong. I just make it part of my routine check in those with impotence.
And of course testosterone, I listed estradiol because in my experience you need about a 10 to 12 fold ratio of testosterone to estrogen. I like estrogen levels to be around more than 50 in men to help prevent dementia. But less than 80, somewhere around 50 to 70 to me is ideal and of course thyroid. So I expanded his chart some in regards to the endocrine function. And then this is pretty much the same as what he had or the authors had. All I added was I moved the PDE5 inhibitors down to after thinking about all of this because you don't need the Viagra if they have hyperprolactinemia or maybe if you pull them off the SSRI and put them on Wellbutrin. Anyway, but it's here.
I put here things that have been shown to help with Peyronie's disease and secondary with erectile function and good studies.
And then the rest of this is the same except I added our P-Shot® and Botox on the regenerative side. If you look at of everything on here, the only thing down here in the other than lifestyle and comorbidity treatment that actually makes the tissue of the penis healthier is in this box. And so I want to expand upon this vacuum device part of the idea because most people don't think about that as being regenerative. And then of course after you pick one or two of these, and then the next thing on his chart was the level three was using intelligently combined therapies.
And many of us already combining Botox with the shot, with the shockwave, with the VED. That's your Rolls-Royce trip to one of our offices. You get a shockwave therapy, followed by a P-Shot® with Botox, and they go home with a penis pump. And to me, that's the Rolls Royce of improving the tissue health of the penis in the United States, where we can't use exosomes. And yes, we cannot use exosomes. If you missed last week, that's still current. Can't do exosomes or stem cells or birth products in the United States. I mean you can, but you can't do it without risking your license—still.
So combination therapies would then be, obviously a lot of people are doing on everything on this list pretty much. And the Botox studies were done, when they were done it was done with people continuing their Viagra. Many of us do everything in this box and the win is that they get to go down on their Viagra or they get to go down on the dose of their trimix until half the dose, or if they're on a low dose, they might be able to discontinue it.
So all of these work in combination with each other. And I put a link in the chat box of this little chart. I'll print it up and make it available on the website. But before I move on, let me see if anybody wants to correct it or add to that. To me, treating sexual dysfunction is, the whole thing used to be, if you understand syphilis internal medicine. Then I always said if you understand testosterone replacement, you really understand medicine.
I think even more than those two, if to really be good at sexual medicine because it's the cherry on top of good health, you have to understand medicine. But if you don't want to do this part of it, the lifestyle part, the hormonal part, at least have some idea of what's been done for your patient. If you're just going to do shockwave and P-Shot®s, make sure that the person's primary care doctor or gynecologist someone is thought about in an excellent way, everything on the top of this page.
Okay, let's see if there's any other comments and then we have an interesting question to answer, but I want to jump back over to the vacuum pump research because I think it gets overlooked and maybe to the loss of some of the benefits to our patients.
First of all, I admitted I had a blind spot. I did not realize that Xiaflex or collagenase had been made not available in Canada and Europe. I never was proud of the fact that they seemed to... Am I reading? I never could get a really good answer about the true incidents of penile fracture went on collagenase, but the best I could tell it was around 2%, which doesn't sound like much, but 2% is one in 50. If our P-Shot® was causing one in 50 people to have a fractured penis, we would already been run out of town. So I think that's what happened basically is, but I haven't figured out why I was blind that it was even happening. But I'm showing you this article where someone in the Netherlands is trying to prove that it should be reinstituted in Europe by doing more research with collagenase.
But then if you look, let's find the, yeah, yeah. So this is my favorite paper showing that our P-Shot® helps Peyronie's disease with a side effect of improving erection by a legend. This was really the pioneer of doing intracavernosal injections. Ronald Virag is a legend, received rewards for just changing urology forever and this is his paper. You guys have seen me wave it around a lot showing that PRP helped Peyronie's disease. The thing that can be confusing for people is this hyaluronic acid part. This was not in the context of a filler, it was in the context of an activator. Regen has a tube that comes with a non cross-linked hyaluronic acid to activate the PRP. So that's the purpose and again, I think emphasizing the fact that PRP needs to be activated. Cell field comes with calcium chloride.
Most of us buy calcium chloride or calcium gluconate separately to activate our PRP. So that's the PRP part of it. But back to the pump part of it, this is one of my favorite papers about the pump and in this paper, those who used the pump twice a day you can see it was 31 patients with Peyronie's disease and they 51 was the average age, 24 to 57 for 12 weeks, which 12 weeks if you notice is a common endpoint for soft tissue. This seems to be where most people grade the conclusion. And so 51% canceled their surgery. These were all people bound to have surgery as you can know, which the side effect is your penis gets shorter and the Peyronie's may come back in a different place because it's autoimmune. So you take away one place, and it comes back in another, not something most people want to sign up for. So 51% satisfied.
The reason I wanted to bring this back up, this is just a straight up pump. If you go back to this guy who was smart man, but he's campaigning to have Xiaflex or Collagenase reinstituted in Canada and Europe. And if you look at the actual percentage, it went from 41% able to have sex before treatment up to 74%. In other words, and part of the study that was with pump part was out. The bottom line was, it was about using a pump. As far as going from curvature too much to be satisfied to curvature to where you're satisfied enough to have sex.
The pump wasn't mentioned here, but the numbers were similar to using the pump in this British Journal of Urology paper. Again, I know lots of people are using the Xiaflex in the states and love it. All I'm saying is that, in my opinion, if we can use Xiaflex, we should be able to talk about the other part of the chart I showed you and be just as excited about everything here and use our shockwave and our P-Shot® and our pump rather than going straight to surgical therapies.
In other words, we're still first class when you look at the numbers. Now back to, we didn't cover... Oh, that I wanted to bring this up again. This was just because I got more questions about it. I'll put a link to this in the chat box. This guy as a sideline to his paper just mentions that in the US we still cannot use, he says be aware of the evolving guidelines. And he just says right here in the paper that, "Exosomes are an air of research, but currently, no FDA approved exosome. None. None. If someone tells you they have a product that's okay with the FDA," this paper came out in this month. So he's backing up what I'm saying here. It scares me when I have people arguing with me. I'm not going to argue, but they say I'm just wrong that their drug rep said it's okay to use our exosome products and not say, oh, okay, well. I guess we just are going to agree to disagree. But that's what this review article said as well.
Vacuum Pump for the Penis—science
Okay, so we covered the chemotherapy, the diabetes, there was another pump article. I think I'll skip over that one though. The bottom line is that I think what the other thing that might... Oh, I know what it was. Let me pull it up. Hold on. There's another one I want to show you about pumps. That's huge. This one. You guys have heard me talk about this I think, but I've never actually shown you the paper where they measured oxygen saturation before an after vacuum therapy with erectile dysfunction after prostatectomy. And not only was the penis more oxygenated post-pump, but it stayed more oxygenated. I'll put a link to this one in the chat box, throughout the day. In other words, it's taking the place of the nocturnal tumescence by feeding blood.
And David Harfield was on here, I don't know if he's on tonight, but he was on, I couldn't find the paper, but there's a paper talking about intermittent hypoxia causing triggering reaction that causes tissue repair and neovascularization after hypoxia.
So not only is it more oxygenated afterwards, both immediately and throughout the day, it could be triggering a regenerative process. And then my theory is that since we know vacuum, this one have nothing, this is me making up something, but it makes sense. Since we're putting vacuum on a tube full of blood, we know that vacuum activates platelets and so we're actually making, in my opinion, small aliquots of activated platelet-rich plasma or activated platelets every time the person uses the pump.
But I wanted you to see this study because that's part of the reasoning behind using the pump. That's part of a penile rehabilitation protocol and many of us are combining the pump along with a low dose daily Cialis and our P-Shot® plus find a shockwave. So there you go. The last thing I think to talk about, let's see if any questions yet.
Yeah, that's a good point. Thank you January. The other thing that people are saying that you should, in my opinion should be, they're adding propaganda to lies. The same reps who will tell you, you should use their exosome product, even though exosomes are not approved, there is no exosome-approved product for IV or intra or injection use in the US, they will make the case that if you're over 40 years old, you're a PRP doesn't work. Which if you're 20 years old and your inaudible 00:28:45 and on high dose corticosteroids, your PRP doesn't work. But the rule of thumb I think makes the most sense as a clinician, is if you can heal from surgery, your PRP is going to do something beneficial because it's the same process. If you can't heal from surgery no matter what the age, then maybe your PRP isn't going to work so much. But whatever the idea about the PRP in the states, exosomes are a risk to your license, currently. Okay, let's see, what else? Any other questions? Thanks January for that reminder. All right.
Press Interviews
All right, let me jump over to the question and some tips about how to deal with interviews. A lot of you guys are interviewing each other or being interviewed by others regarding our procedures. So I can run through. If you guys know me, anybody who knows me knows that at heart I'm the most introverted introvert that I know. I mean, there have been times in my life when I avoided going to public places, almost agoraphobic. But on one-on-one I always cared for people and that came naturally to me and just for some reason was intrigued and enchanted maybe by almost everybody. But I wasn't too hip on talking in public. I just make myself do it because it needs to be done and I've enjoyed the people I've met and I've been on the news way more than I would've ever anticipated in multiple countries and in states all over.
And so these are the tips from the introvert who did it and had to figure out a way to do it and make it work. So I'm not a media coach, but this is what has worked for me. So we'll get to that. The general tips are at the bottom of here and I'll expand on those. But these are common questions that people are asked that were sent to me by this person who'll be interviewed tomorrow.
Etiologies for ED best treated with the P-Shot® procedure
So what's the most common ED causes best treated with a P shot? Your rule of thumb is that what we are doing with PRP anywhere is we are having a local effect on the tissue. So any etiology that is not local, we're not as likely to help it. So if someone has low testosterone level and their hypothyroid and depressed and on beta blockers, then all we're doing with the P-Shot® is making the tissue of the penis healthier, maybe it won't work so well. If you go... I want to show you guys this real quick because a lot of this, and we'll come back to the rest of this. Let's see, hold on a moment.
So if you go to our Priapus Shot® website, if you've been in the group a while, you may not have seen this. But I put a more structured course in here that I think is probably helpful for to go through, even if you've been in the group for a while. Let me just go to the website, and I'll show you. When you land, you'll usually be on this dashboard. And this was all that was here. It was more like a filing cabinet, how to do the procedure, the marketing part, and the survey, et cetera.
This is where all the consent forms live and where to buy your stuff, you get; it’s self-explanatory. And people used to have to jump around. Usually, they started here, learned how to do the thing, and then went back to the rest as they needed it. The thing that's different is I added a formal guide that takes you through that filing cabinet in a fairly logical way. And these lessons are often just a few minutes long.
Here's the first lesson is just to recommend people sign up and come to these journal clubs, and I show them where to do it because I know that the people who come to these journal clubs are more involved, the ideas stay fresh in their minds, they get better results. They market better and see more people, make more money, and have more people crying in gratitude in their office.
So these first four things are just how preliminaries know where the research is. Teachers can't overemphasize teacher staff this phone script. And so I lead you through every... That's my son back when he was a high school kid. I lead you through the filing cabinet, but everything that's in the course is in the filing cabinet. All right? And in this filing cabinet is the answer to almost every question that might be asked.
And then, if you get really stuck, the other thing that's helpful is to just put your question over here in the search bar right there, and it'll bring up these journal clubs. If I put here Peyronie’s, then it will bring up where we've talked about Peyronie's in the past and previous journal clubs.
But then back to the question I just wanted to show you because that structured course is a good thing because a lot of things that are helpful in both the marketing and the pearls for doing the procedure sometimes get overlooked in the more haphazard way that I had things set up. So I wanted you to see that's available. Everybody that's in the group can log in and do that.
Now, back to the questions and how to deal with the press; get you back there.
So with this first one. The most common causes that would be best treated would be ED that's mild to moderate because those are the people less likely to have iliac disease. This would be someone who's erectile dysfunction score is going to be somewhere around 10 or more. And another practical way to think about it is, if they get nothing, no tumescence at all from taking Viagra, no morning erection at all, no morning tumescence or they've had diabetes for 30 years, then P-Shot® alone is not likely to help them. Now that we're adding Botox in, I don't know, I have less experience with the combination, but just for the P-Shot®, because some of those, or actually all of those who responded in the double line placebo controlled studies were not responding to maximal doses of PDE5 inhibitors. So maybe we'll do better now that we have that combination.
But in general, two things that I don't like treating, someone who has had long-standing ED with no tumescence, no matter what they do, and someone whose main goal is to change the size of their penis significantly. I've found those two people difficult. Your easy-hanging fruit is the person who's got some tumescence. They may even be on one of the injectables or the Trimix or maybe they're on a higher dose of Viagra, but things are working; they’re just not working as well as they were. They'll be able to cut their dose in half or come off of it.
Nothing else does that.
You just have to go up on the dose until you need an implant, or perhaps your shock wave might help. But as far as there's not a lot out there except of our regenerative therapies other than just going up on the dose and people can become unresponsive to the trimix sometimes pretty quickly. Then in other words, our easy stuff would be very difficult otherwise.
So you got that and then you have, so the person who's responding but do something else, but they want things to be better. Also, Peyronie's disease, like in sclerosis in men and they're trying to recover from prostate surgery, but were able to have erections before the surgery that's worth the shot. Your lowest hanging most common treatment is going to be the person who is responding to some pharmacology but wants to go down on the dose or they're not on Viagra but they want to avoid it or Peyronie's or recovering from prostate surgery. That's your best candidates as far as the maintenance go and how often, most people are coming back for the past decade that I've been doing it. T
hey usually show up about every 18 months.
If they're wanting to see if they can make things improve or perhaps the first procedure was not as helpful as they would wish, I'll let them come back as long as every time they're coming back it seems to be improving. I had a man who flew from New York City down to the Gulf Coast here to see me in Alabama five times for loss of sensation. Each time he thought he improved it until the fifth time didn't seem much better than the fourth, so we stopped and he was happy.
Most of the time people are getting their maximum benefit, unlike with a hair, they seem to see their maximum benefit after the second injection and they show up every year to 18 months. And the other question that gets asked along with that is, well it is almost an I got you kind of thing. If you have to keep doing it and then maybe I don't want to do it. Well, what you're doing of course is you're slowing the inevitable aging process with doing nothing. Research shows most men lose about 50% of the endothelium. Their biceps are shrinking, but their penis is also shrinking by and they lose about half by the time they're 65.
But that doesn't stop. We reverse it with the P-Shot® and then it progresses again from a new set point. So we just try to stave off the inevitable eventually, unless something big happens, we're all dirt on this planet and we just we're slowing the process down for that one part of the body.
Tips for Interviews with the Press
Okay, so general tips when being interviewed about any of our procedures, I'll go through this pretty quickly, and then we'll end the call. But this would also, I think, even if you're not being interviewed, these points would be helpful on the website, podcast, and your own videos.
These are points that I think allow you to be truthful, to be complete and yet, and so not lose your credulity, yet you are still able to give genuine hope. So I'll run through them things. First of all, before I talk about anything to do with sex, I like to always, even though most of us love the pleasure of sex, I like to bring it to a higher level, which is that sex also relates to creativity. It relates to Riner Maria Rilke who wrote Letters to a Young Poet, and thought it was directly related to your creativity.
Next Hands-On Workshops with Live Models<---
poets and philosophers have said the same thing. Thoreau said the same thing (see the last chapter of Walden). And so your creativity is related to it. If you're a salesperson, you sell more if you have a good sexual function. If you are a leader, if you're a politician, if you are an athlete, if you're a mother, if you're a grandfather, sexual function gives you more energy. It gives you more sparkle to your personality.
Walt Whitman said, "Whether you're blackening a shoe or you're writing a poem, it's all about sex."
And in when you take it in the larger sense of the word, outside the bedroom, but in relating to creativity almost on a spiritual level, that sex is involved and truly is involved in pretty much everything. So that's that part of it. The other part is that, it's about relationships and family and of course family is part of the fiber of our society and our lives.
And when that falls apart, then you're dealing with economical and psychological disaster often. So it has, as part of that fiber of family, and I like to bring it as quickly and as succinctly as I can, pull that into the conversation. Now, I'll get to more keywords in a moment but just realized that you can do that. It's worth it, even though it is somewhat angering, it's worth watching. It doesn't matter what TV news channel you like to watch, it's got nothing to do with politics because they all do it.
But watch politicians, when someone asks them a question, you can't watch them for more than a minute without seeing it happen that they don't want to answer, they will quickly talk about whatever they want to talk about and use the question more like a bell to talk than actually a signal for what topic they should dive into.
Now, obviously you take that to too far of an extreme and you're disingenuous. But if for example someone says, "Well, does this make sex better?" Then my answer would be, absolutely when this works, it can make the pleasure in the bedroom tremendously better. But before we talk more about that, just realize that sex, it has much more to do with our lives than just sexual pleasure with the lights out has to do with our, than I would clinge into all the things I just talked about.
So you can start where they are, where the question is. And that brings me to this point, number three is that when you're being interviewed or when you're just going to do your own videos, podcast, whatever, I like to have a list of keywords that I'm going to say. You can ask me the weather and if I'm going to talk about the P-Shot®, I'm going to bring it up.
Or if I'm going to talk about how it relates to family, even if you ask me about orgasms, I'm going to talk about and orgasms create an emotional bond between, you get it. So you can always bring your topic in. But I like to rake those keywords out often the night before or so oftentimes it's just a few minutes before and then right before I have to go on camera or do my video at home, wherever, I'll look at those keywords. If possible if I'm home making a video, I'll just stick them up on the screen somewhere where I can look at them to remind me.
The next thing is that, really, I said to someone you love, but when you're doing an interview podcast or the news, there's really three people you're talking to and everyone else is just listening in. At least the way I conceive of it.
The camera is someone that I love that could relate to the topic. So many of I have a baby sister who's, in my opinion, the biggest hero I know at the moment who's struggling with breast cancer. And so if the topic was breast cancer, I would imagine that the camera lens is my baby sister. But then there's also the host or hostess of the show or the podcast or whatever. And so I would be as connecting as I can to that person.
You could do an interview and you could say all your words and never connect to the person. You need to be in the present moment and connect to the person you're talking with. And I would add to that brag, I like to always brag on their courage because even now, even though you have all sorts of people doing outrageous things on Twitter or whatever, it still takes a lot of courage for most people to talk about sex in an open manner and risk their reputation doing it. Which brings up the other idea, which is that sex is still taboo similar to psychiatric problems.
And so I always brag on the host who's interviewing me for having the courage to talk about it. And if I get the chance right up front, thank you. I realize this takes a lot of courage to talk about sex.
Sex as a medical physician or as a patient is similar to say schizophrenia. If you break your arm, you have people sign your cast, you take a picture of it, put it on Facebook. But if you had schizophrenia and auditory and visual hallucinations, you may not put that on Facebook.
The same thing even with major depression, people say, oh, you've got a nice life and pretty car and healthy family. You don't have... There's not a lot of empathy it seems to those problems. And people will say things they would never say if you had cancer or congestive heart failure. You'll see snide remarks.
Women seem to be the most vicious against other women when they on the chat forums and such, you'll see women saying stuff like, "Oh, you just need a man with a black Amex card o,r" stuff like that. Things that they would never say to each other about something having to do with other physical ailments.
So the keywords and the outline that you guys, if you've been to my workshops, you know my outline. And so that will be incorporated into my keywords. What's the problem? How's it affecting things other than secondary effects that are affecting their life? What's been tried? What's new? And you try to make something, even though the P-Shot® now has been around for a decade, there's new research, there's new ideas about how we're combining it. So there's new, now we're combining it with Botox. Shockwave is becoming more prevalent. So there's always something new. And part of what I hope to provide here is new things for you to talk about. So it does stay fresh.
So it's what's the problem? What's been tried? What's new? What's not possible? And what is possible? And tell me what to do. And I like to have something set up someplace to send them a website to send them to, a phone number. And now a lot of people are texting something somewhere, but something where they can engage with you afterwards and get something free.
Send me an email here and we'll shoot you our latest research. And I'm not a big fan of something off because to me it sounds too much like a used car salesman. I like giving away something educational if they'll reach out to me and then in the process of giving it to them, I collect their email address and now we have a chance to establish a relationship. I don't usually try to make the sale to get to my office on the interview, I make the sale to get to my website to get something for free in exchange for their email address.
So that's the thing that I put for the thing to do. Then I always include something about you just lose credulity if you're all roses. So always bring up something about how this doesn't help everyone. And if you've got something like if you, let's say if it was the P-Shot®, if you have prostate cancer, we can't fix that with a P-Shot® or if you're trying to double the size of your member, we can't do that, but we can do this, this, and this. And I think it balances out and gives you more credulity.
So then this is a question, it doesn't come up so much now because thankfully most people have figured out the answer to it. But it should roll off your tongue so quickly, because every now and then, when I was on the doctor's show, it was the very first question. It took a deep breath. I didn't have to try to think of what the answer was. I mostly had to take a deep breath. Because the fact it was asked by a host on our hostess, one of the celebrities on the doctor show.
Maybe she was asking it for the benefit of her viewers. So I'll go with that. Anyway, her first question was, or comment was, this is not approved by the FDA.
So the thing that should immediately come out of your mouth is that the FDA doesn't regulate procedures, they regulate drugs and devices and they don't regulate body fluids. Plasma is a body fluid. They don't regulate it anymore than they do saliva or urine, but they do regulate the device we use, which is part of the reason for the price involved because we use a device that's approved by the FDA to prepare plasma to go back into the body. That's the answer to that question, should it happen?
And then just having some knowledge of our research and all of our research lives at whatever the procedure is, .com/research. So for the P-Shot®, it would be priapusshot.com/research, oshot.com/research vampirefacelift.com/research. So you might want to zip over some of that before you do your interviews and some of it will, you might even pick one or two that you bring up, never talk down.
And many of you've heard me talk about this before, but in my opinion, you want to be understood. But if you don't, let's say use the big words. If you don't say a few things, they don't really understand, they're not going to think you're smart. So be as smart as you are. You're no longer on the bus. If you're like me and you rode the public bus and you started talking about the Shakespeare you read yesterday in the library, you might be considered a smart ass and wind up having to have a fistfight. So you possibly have learned not to be as smart as you are. And I have to remind myself sometimes, it's okay, it's actually desirable that oftentimes if I'm smart as I am, I still will not be the smartest person in the room.
And so your patients are smart and smart or not unless you say at least a few things they don't quite understand they might have trouble thinking you understand what you're talking about. They need to hear that. Okay, I think that's all I have for tonight. Let me see if there's any questions. I don't see any. Let me see. I might want to put a couple more links about the research whenever and unless more questions pop up, we'll call it a night. Let's see, oxygen saturation, yeah I'll put that one in there. And think with that, we'll call it a night. So if you click on that, it'll be there when we end it.
Always honored when you guys come out. I hope you found something helpful in tonight's call.
Goodnight.
References
Cayetano‐Alcaraz, Axel Alberto, Tharu Tharakan, Runzhi Chen, Nikolaos Sofikitis, and Suks Minhas. “The Management of Erectile Dysfunction in Men with Diabetes Mellitus Unresponsive to Phosphodiesterase Type 5 Inhibitors.” Andrology 11, no. 2 (February 2023): 257–69. https://doi.org/10.1111/andr.13257.
Geelhoed, Jeannette P., Olivier Wegelin, Ellen Tromp, Bert‐Jan De Boer, Igle‐Jan De Jong, and Jack J. H. Beck. “Improvement in the Ability to Have Sex in Patients with Peyronie’s Disease Treated with Collagenase Clostridium histolyticum .” BJUI Compass 4, no. 1 (January 2023): 66–73. https://doi.org/10.1002/bco2.185.
Raheem, Amr Abdel, Giulio Garaffa, Tarek Abdel Raheem, Michelle Dixon, Amanda Kayes, Nim Christopher, and David Ralph. “The Role of Vacuum Pump Therapy to Mechanically Straighten the Penis in Peyronie’s Disease.” BJU International 106, no. 8 (2010): 1178–80. https://doi.org/10.1111/j.1464-410X.2010.09365.x.
Wikramanayake, Tongyu C., Nicole I. Haberland, Aysun Akhundlu, Andrea Laboy Nieves, and Mariya Miteva. “Prevention and Treatment of Chemotherapy-Induced Alopecia: What Is Available and What Is Coming?” Current Oncology 30, no. 4 (March 25, 2023): 3609–26. https://doi.org/10.3390/curroncol30040275.
Virag, Ronald, Hélène Sussman, Sandrine Lambion, and Valérie de Fourmestraux. “Evaluation of the Benefit of Using a Combination of Autologous Platelet Rich-Plasma and Hyaluronic Acid for the Treatment of Peyronie’s Disease.” Sexual Health Issues 1, no. 1 (2017). https://doi.org/10.15761/SHI.1000102.
Yang, Shangyang Christopher, James M. Weinberger, Robert H. Shahinyan, Gary K. Shahinyan, Jesse N. Mills, and Sriram V. Eleswarapu. “Regenerative Therapies for Erectile Dysfunction: The Influence of Direct-to-Consumer Marketing on Patient Interest.” Translational Andrology and Urology 12, no. 4 (April 2023): 586–93. https://doi.org/10.21037/tau-22-309.
Next Hands-On Workshops with Live Models<---
Relevant Links
-->Apply for Further Online Training for O-Shot®, P-Shot®, Vampire Facelift®, Vampire Breast Lift®, Vampire Wing Lift®, or Vampire Facial®<--
-->Next Hands-on Workshops with Live Models worldwide <--
Dr. Runels Botox Blastoff Course<--
--> IMPORTANT (ONLY) IF YOU ARE NEW TO THE CMA: Please take any relevant online tests so that we can immediately list you (and your clinic) on the directories and start supplying you with other helpful marketing and educational materials. Testing takes an hour at most (including watching the videos. If you want to expedite the testing, you can simply call the CMA headquarters (1-888-920-5311 9-5 New York time Mon-Thur; 9-12 Fri) and one of our business consultants will log you in and walk you through where to find the study materials and the tests. If you are already on the directories for the procedure(s) you provide, then you already took the tests or did hand-on training with evaluation by your instructor.



Cellular Medicine Association
1-888-920-5311